SARPEP
Early intervention
Early intervention
The first episodes of psychosis usually occur during the transition phase between adolescence and adulthood. This is a critical period whose interruption can significantly compromise the future of the individual. This is why teams of professionals are dedicated to early intervention for psychosis, in order to limit the negative effects on the evolution of symptoms, the person’s functioning and response to treatment.
SARPEP
SARPEP
The implementation of intervention programs for first episode psychosis (FEPP) across Quebec is now a priority for the MSSS, well framed by a reference framework. International experience shows that such large-scale implementation is a considerable challenge.
To meet this challenge, we have set up a learning system to evaluate the implementation of FEPP in real time. This system makes it possible to monitor and guide interventions, thus ensuring continuous improvement in the quality of care for people with FEP and optimal support for care teams.
Learning Health System (LHS) [SAR]
Learning Health System (LHS) [SAR]
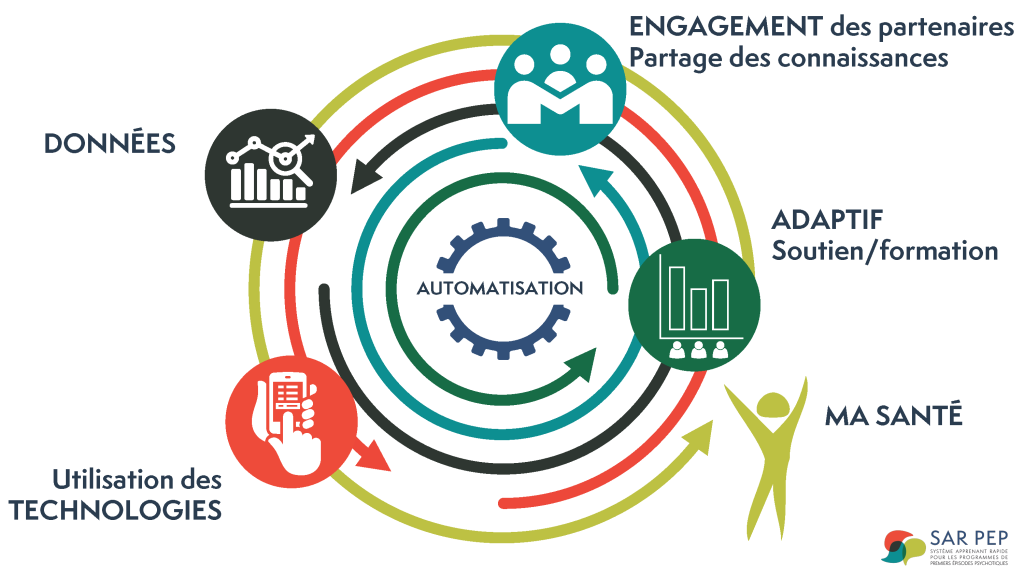
A rapid learning system (LS / SAR) is defined as an approach where « science, computing, enhancers and culture come together for continuous improvement and innovation ». By integrating best practices into the care delivery process, the new data captured generates knowledge as a critical by-product of the strategy.
A LS can significantly improve the uptake of clinical guidelines and evidence-based medicine in clinical settings, as well as the translation of knowledge into practice. LS has been shown to foster innovation, link evidence to practice, and improve the quality of health care delivery in a variety of contexts related to physical and mental illness.
History
History
In the context of the rapid expansion of FEPPs and the publication of the MSSS Reference Framework, the SARPEP project was launched in 2020 in 11 FEPPs in Quebec. These 11 programs were selected to provide a representative sample of FEPPs, taking into account their environment (urban vs. rural) and their affiliation (university or not).
The pilot phase established a systematic data collection process, generating feedback for teams and bringing together a community of practice committed to improving care. The pilot phase proved to be particularly effective in demonstrating the feasibility and acceptability of implementing such a rapid learning system through the 11 participating FEPPs.
Since then, impacts on practices and decision-making at the local and provincial levels include:
- Adapting the standards of the reference framework to the realities of the FEPPs
- Improving the referral process and access times
- Reducing exclusion criteria
- Increasing the continuing education of professionals
- Integrating peer support
The PAIRPEP project was launched in 2023 to promote the development of peer support and family peer support within FEPPs in Quebec.
Today
Today
Having become a partner with the MSSS, SARPEP has been deployed to date in 20 FEPP clinics across the province.
The next step is to expand the initiative to all 33 FEPPs in Quebec, building their capacity to provide evidence-based care, track their performance, set improvement targets, make decisions at the local and provincial level, and foster collaborative learning and multi-stakeholder interactions between clinics.
Finally, SARPEP serves as a model and inspires the development of other SAR initiatives, both in Quebec and around the world.
SARPEP Indicators
SARPEP Indicators
Based on in-depth literature reviews, expert recommendations and a systematic assessment of the environment, the SARPEP indicators were selected in consensus with all project stakeholders. These were identified as being both the most relevant in terms of impact on young people and the most realistic to improve.
FEPPs should facilitate well-known, easy and timely access mechanisms to assessment and initiation of treatment.
This indicator includes:
- Direct or non-direct process
- Self/Community Referral Sources
- Inclusion and exclusion criteria
- Number of contacts prior to access
Early intervention involves offering appropriate treatment including the offer of all interventions that have been shown to be effective.
This indicator includes:
- Type of specialists providing interventions
- Cognitive Behavioural Therapy
- Family intervention
- Employment and Education Support
- Integrated Addiction Services
- % Antipsychotics & Clozapine
It is essential that FEPPs aim to ensure a full commitment of the person to be involved in his or her follow-up. The more sustained the commitment, the less likely it is that relapses will be rapid and frequent, and the less significant the cognitive and social damage that will result will be in the short and medium term.
This indicator includes:
- Adaptation to specific needs
- Youth friendly environment
- Outreach practices
- Disengagement
The FEPPs must also aim for the involvement of the family and friends since they are essential partners in the follow-up.
This indicator includes:
- Types of Interventions offered
- % of families involved
- Number of visits
- Family Member Satisfaction
Reducing the time to assessment is intended to reduce the duration of untreated psychosis (DUT) and maximize the youth’s commitment to their care. A shorter DUT is associated with a better symptomatic and functional course.
This indicator includes the delay between referral and:
- 1st contact
- first evaluation
- start of care
All staff must obtain regular continuing education to develop and maintain their expertise, and thus offer quality early intervention services.
This indicator includes:
- Number and type of continuing education events attended by clinicians
- Supervision/Mentoring
Adequate ratios ensure the accessibility and intensity of follow-up required to meet the needs of young people.
This indicator includes:
- Patient-to-Case manager Ratios
- Patient-to-psychiatrist ratios
This indicator includes the user’s evaluation on:
- Their mental health
- Their recovery
- Their quality of life
Stakeholders
Stakeholders
SARPEP values the perspective of people with lived experience by collaborating with patient and family partners from different FEPPs.
SARPEP involves not only team leaders, but also other health professionals, including psychiatrists, supervising more than 170 health professionals and 60 psychiatrists.
At least one manager per FEPP is involved in the project.
SARPEP collaborates in partnership with the MSSS and AQPPEP to guide initiatives and policies, while ensuring that the specific needs of FEPPs are taken into account.
With six principal investigators and a dozen co-investigators from various university research centers, SARPEP benefits from a diversity of expertise.
Feedback on data
Feedback on data
Personalized results are continuously disseminated to SARPEP users in the form of popularized feedback, in order to offer recommendations for the improvement of the FEPPs and also of SARPEP itself.
Capacity building
Capacity building
SARPEP contributes to capacity building and adapts to the changing needs of each participating FEPP by developing clinical-administrative tools and expert-led community of practice activities. All the tools are accessible to the participating sites via our media library.
Clinical-administrative tools developed:
- Common database
- Appointment cards, posters and practical information sheet for satisfaction collection
- Checklist, plan and brochure on the transfer process
Topics previously covered in community of practice activities:
- Reduced access times
- Post-FEPP Transfer Process
- Family involvement
- Youth engagement and disengagement
- Youth satisfaction
- Facilitating direct referrals
All tools and knowledge exchanges are accessible to SARPEP members in our media library.